The Act of Diagnosis
2018 – 2019By all accounts, we’re in the midst of a mental health crisis. But what is a mental illness, and who decides? On paper, the answer is surprisingly simple. The bible of the field is The Diagnostic and Statistical Manual of Mental Disorders (DSM). Now in its fifth edition, the thousand-page tome is maintained by the American Psychiatric Association. Its scheme of diagnosis is legion: insurance companies, the Social Security Administration, the IRS, the Department of Education, and nearly every other official body relies on the DSM.
But most practitioners view the DSM as fundamentally flawed. In 2013, the National Institute of Mental Health, the world’s largest funder of mental health research, went so far as to roundly reject any future studies using the DSM’s categories. Yet the DSM persists. It’s entrenched, and its absurdities (and frequently even its existence) are invisible to laypeople.
Process
I began this work by conducting interviews with practitioners and the diagnosed, in order to get a better understanding of their relationship and feelings toward the moment of diagnosis. I then designed objects based on those interviews, objects designed to amplify what I was hearing. I brought those artifacts back to later interviews, and continued the cycle of iterative, provocative making.
Diagnosis Horoscopes
The similarities between diagnosis and fortune-telling were a recurring theme in my interviews. The word prognosis is literally “foreknowledge,” so this connection is not altogether surprising. Inspired by this finding, the first objects I produced were a series of six “diagnosis horoscopes.” I picked common diagnoses, from depression to Borderline Personality Disorder, and created scrolls for each.

The main text of each scroll is a mix of verbatim formal lingo from the DSM and the woo-woo nonsense that typically appears in a horoscope. For example, the Bipolar-II scroll notes the fluctuation between hypomanic and depressive states, but theorizes that the cause may be “rich blood.” It suggests exercise, and leveraging mania to get ahead on household chores. At the bottom, I added some adapted versions of standard horoscope tropes – lucky numbers, famous people with the same diagnosis, and so on. The “lucky element” for Bipolar-II, for instance, is the mood stabilizer lithium.
I’ve referred to the horoscopes as a “self-probe”: they helped me understand and explore the tone of the project. They walk the line between absurdity and reality, nonsense and helpful advice. The decision-making process behind them was a huge help in cementing my design principles.
The Idiognosis Machine
The cut-and-paste style I used in the horoscopes appeared to be quite successful. Along the way, I noticed that many of the criteria in the DSM were so generic that almost everyone has experienced them. For instance, being “often touchy or easily annoyed” and “spiteful or vindictive at least twice within the past 6 months” are both symptoms of Oppositional Defiant Disorder. Finally, a series of recent studies point to marked differences in word choice and tone of voice in depressed individuals. This research was promptly massaged into a patent by none other than Amazon: future Alexa home assistants may automatically monitor your mental state based on your speech.
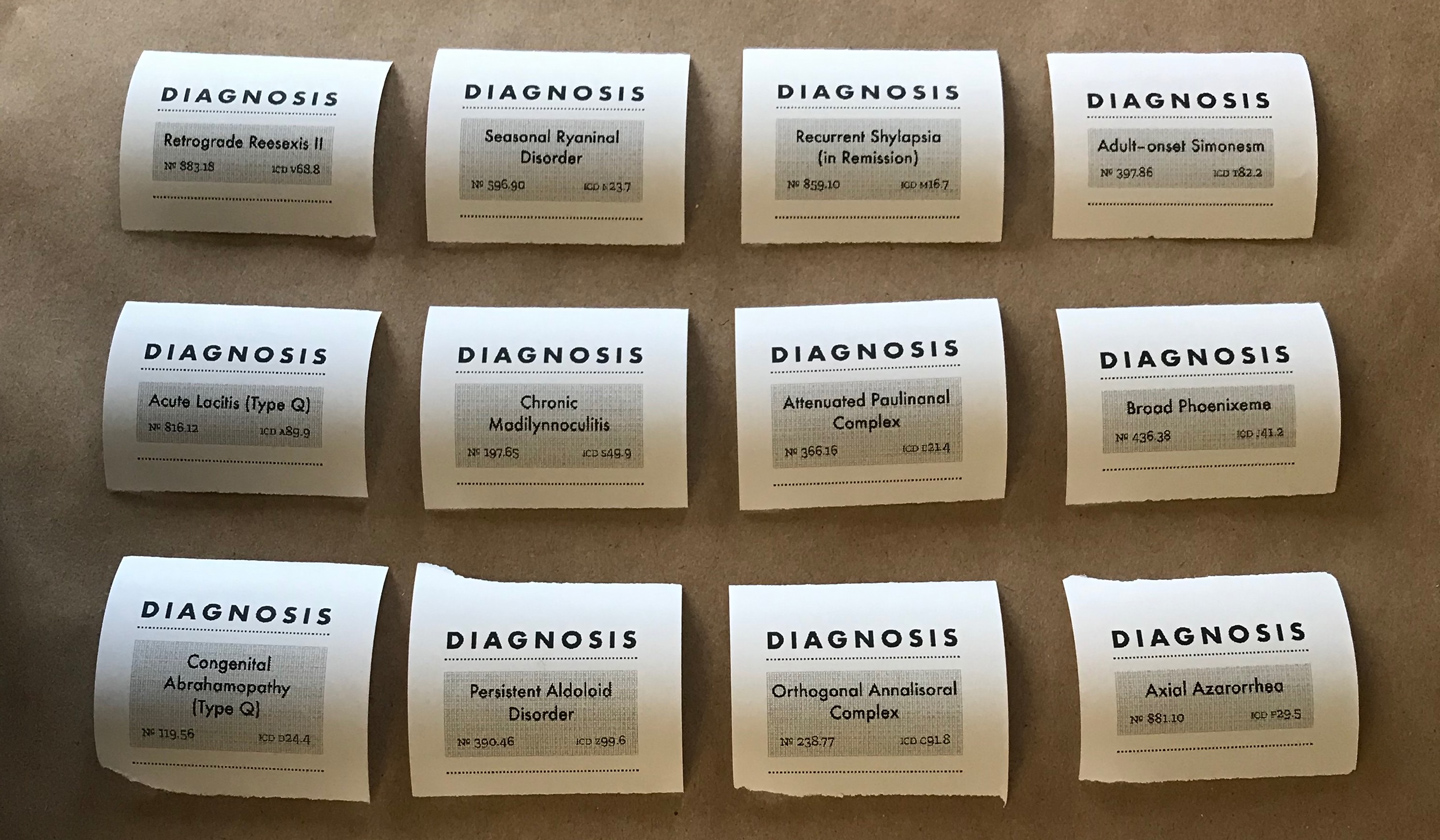
With those touchstones in mind, I created the Idiognosis Machine. Idiognosis is a neologism, formed from the prefix idio–, meaning personal or distinct, and gnosis, knowledge. A user enters her name on the device, and is guided through a series of fake biometric inputs: fingerprint, voice analysis, retina scan, and smile detection. After briefly “processing” the data, the user receives her individualized diagnosis on a printed receipt.
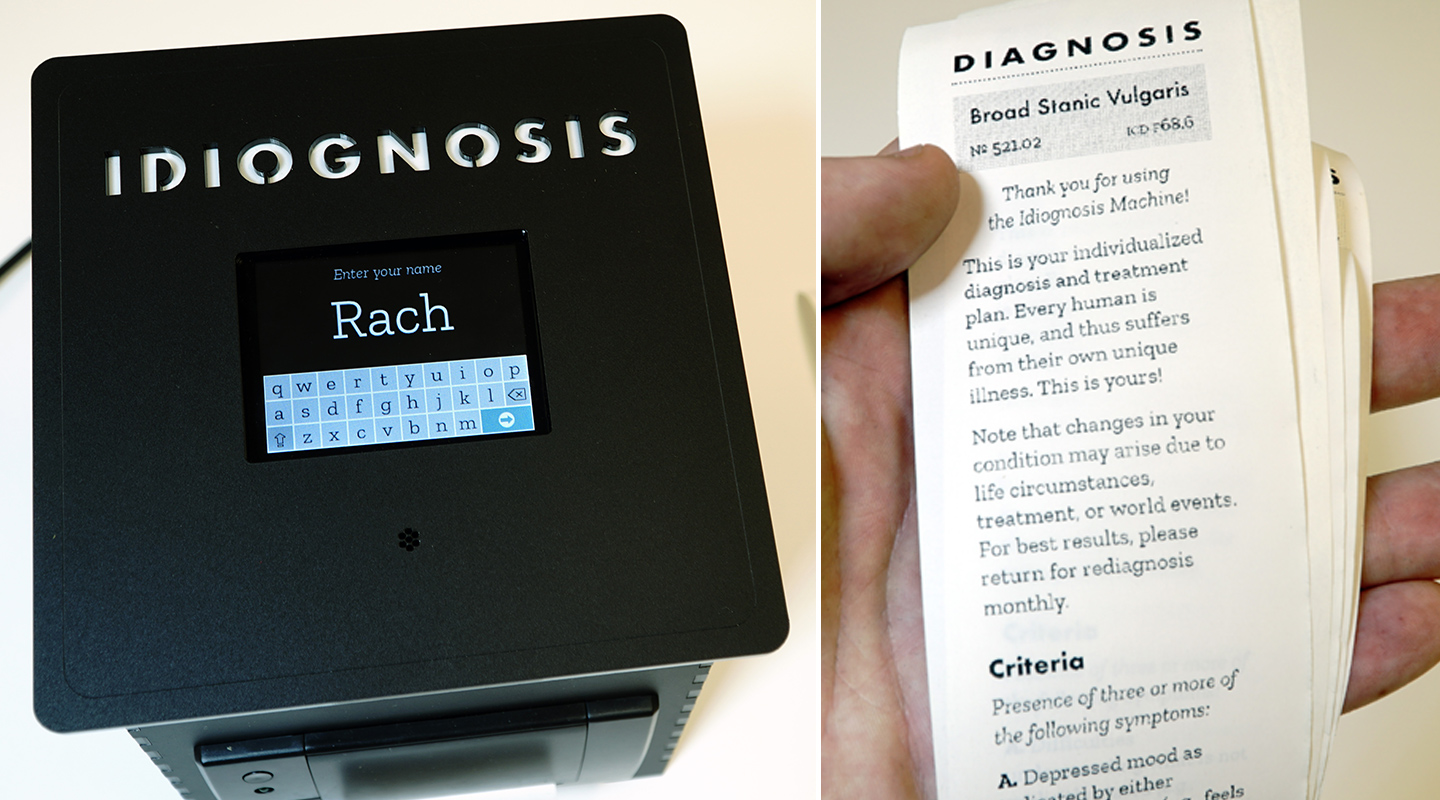
The diagnosed condition is given a unique name, generated algorithmically based on the user’s own name. A list of criteria for the condition is randomly assembled from a subset of several dozen criteria taken verbatim from the DSM. I selected ones that struck me as particularly common facets of the human experience. Next there is a “Risk & Prognosis” section, which again features text chosen from the DSM, particularly vague or foreboding forecasts. Finally there’s a “prescription,” composed of a number of commonly suggested treatments for general wellbeing.
I’ve deployed the machine on a number of occasions, proctoring participants through the examination and asking them questions about their diagnosis. Owing to the particular subset of criteria I picked, most people reported that they did indeed suffer from their eponymous condition. There was general disbelief that the criteria could possibly be symptoms of real diseases.
The DSM-5 Exhaustive Version
The final object I created is the culmination of my newfound fixation on the text of the DSM. The criteria for conditions in the manual are given in a checklist-like form: “you must have x of the following y symptoms,” and so on. I became curious about exactly how many distinct experiences could lead to the same diagnosis.
I chose Major Depressive Disorder (MDD). A diagnosis of MDD under the DSM‐5 requires meeting five criteria. The first of these criteria lists nine key symptoms of the disorder, at least five of which must be present. There are 227 possible ways to satisfy that criterion. Factoring in a number of other twists (the severity and course modifiers), there are 4,767 unique combinations of symptoms that can culminate in a diagnosis of MDD.
That’s a huge number (and is in fact still an underestimate — the definitive count is over 1.2 million). But the point isn’t “how could a practitioner possibly make a diagnosis of MDD”: no matter how big the combinatorial expansion, the checklist format is easy to follow. Instead, the number should prompt us to consider how we condense such a vast array of human experience into one label.
But how does one make such an epistemological problem visceral?
I wrote a program that stepped through each of the 4,767 combinations, assigned it a unique code, and laid out the text of its corresponding symptoms and modifiers. I arranged this text into books and had them printed. The result is a series of eight volumes, each roughly 800 pages. This set of the MDD diagnoses is part of a larger, hypothetical, and obviously incomplete work I’m calling the DSM-5 Exhaustive Version, or DSM-5 Ex for short.
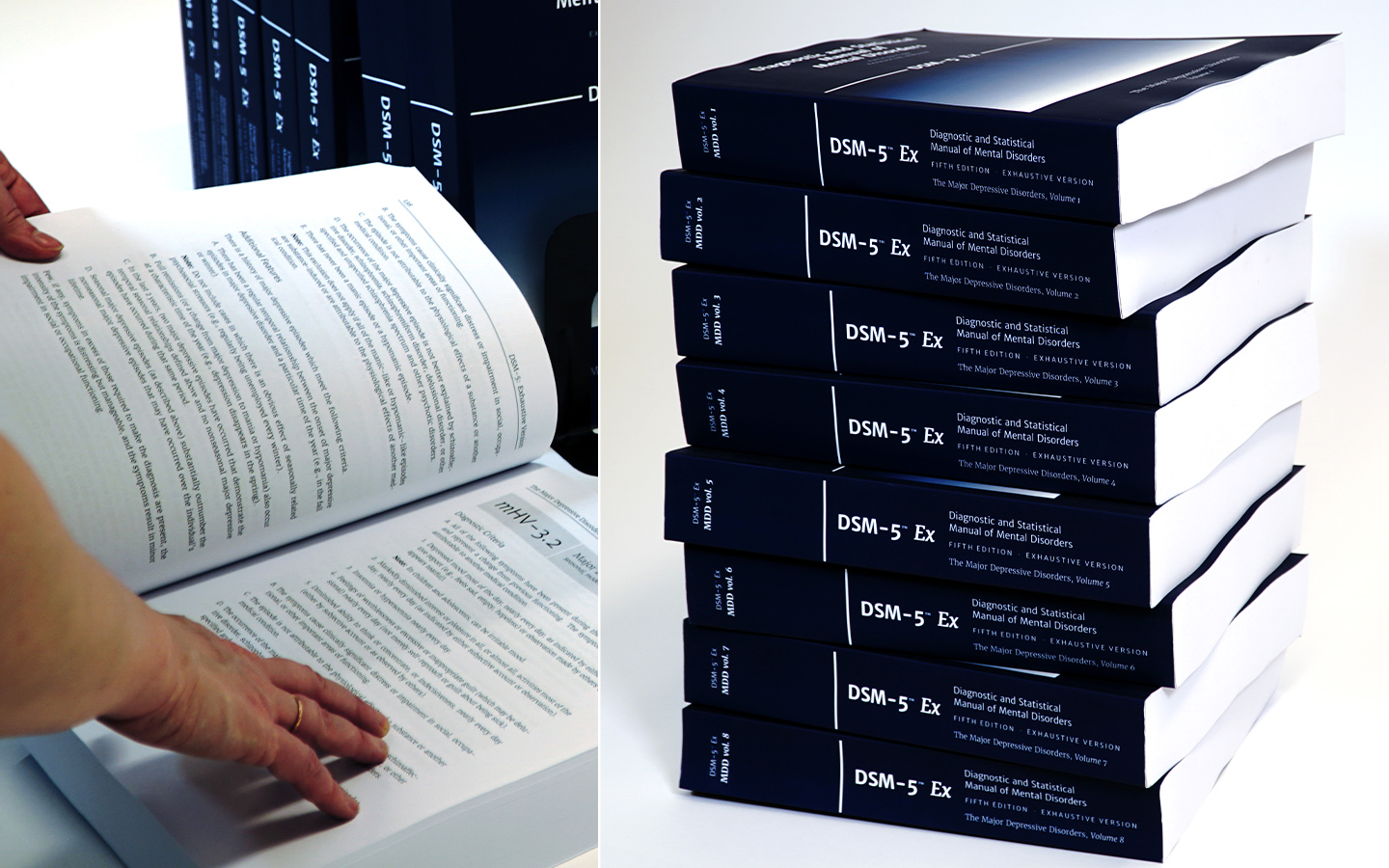
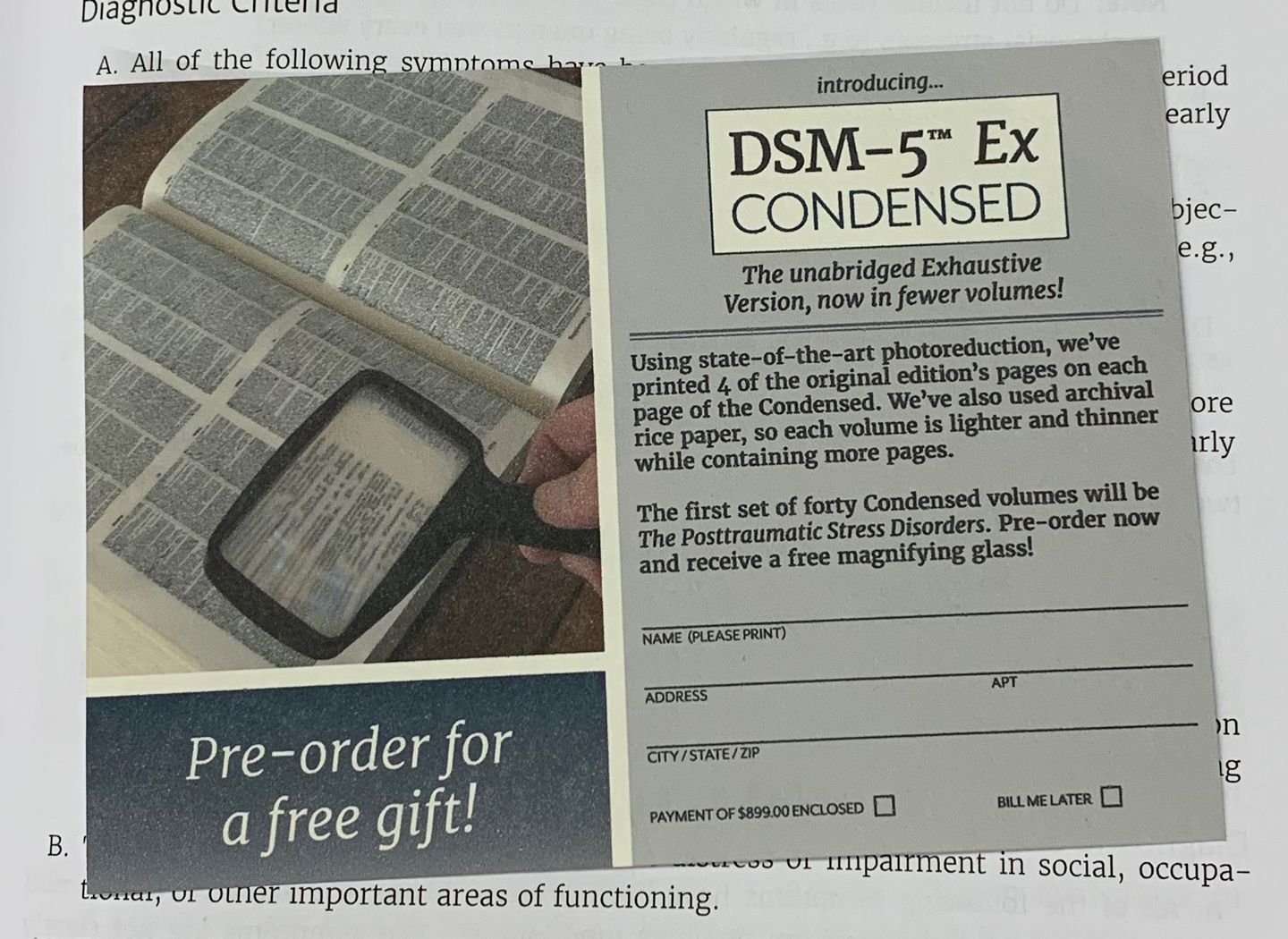
I wanted the books to seem like plausible products, like a new companion series from the American Psychiatric Association. To that end, I designed the cover and interior layout to look very similar to the DSM-5. I also included a mail-in order form in each book for the forthcoming DSM-5 Ex Condensed, a version with four shrunken pages of the original printed on each page. The flyer advertises a special gift for pre-ordering: a magnifying glass.
In interviews, the books did what I hoped: they helped people see that the idea of a monolithic depression is wishful thinking at best. My interviewees pondered which particular depression they have, and whether they may have had many over the course of their life. That critical distance, the ability to other ones suffering, is a vital step toward healing.